














Project Description
Michael Murphy and Alan Ricks are cofounders of Boston-based MASS
Design Group, which also has offices in Port Au Prince, Haiti, and
Kigali, Rwanda. They, along with project architect Sarah Mohland,
discuss the process of designing the first-ever cancer treatment center
in Rwanda.
The cancer center is part of a 15-year master plan for this
rural site. How does the new building fit into the work you’ve already
done there?
Michael Murphy: Our partners,
Boston-based Partners In Health, as well as the Ministry of Health of
Rwanda who run the Butaro District Hospital [which MASS completed in
2011], have a commitment to bringing the best healthcare that they can
to the poorest communities that they serve.
A lot of the funding for healthcare in emerging economies in the Global
South aligns with communicable diseases, such as tuberculosis, malaria,
and HIV. Partners in Health is now looking to the future, to
noncommunicable diseases such as cancer, obesity, and diabetes—the kinds
of things that start to affect people as they live longer. And so they
chose to start what is now the first outpatient cancer center in East
Africa, I believe—the first cancer treatment in Rwanda for sure.
Is it drawing people from a much wider area because of that?
Murphy:
It will certainly draw people from all over Rwanda … as the referral
center for cancer. [Also] I think, ambitiously, [from] the neighboring
countries, the Congo and Uganda, which are in close proximity.
What’s been the larger impact of this center on the local community?
Murphy:
The economic impact of the hospital has been substantial. When I first
got to Butaro in the beginning of 2008 there was no electricity in the
town; there were mostly empty businesses. Not even six years later,
there’s a hydroelectric dam in town. In the whole village below the
hospital, there’s lots of fresh coats of paint on businesses. A Bank of
Kigali has opened up there, not to mention middle-class families are
moving to this community because there’s ongoing work at the hospital
both in terms of service, nursing, as well as in construction.
I know that this project has also involved developing construction skills in the local population, building infrastructure.
Murphy:
One of the privileges of getting to invest more than five years into
this one site is that we’ve been able to grow relationships with a
variety of team members. MASS is bringing expertise, and that’s being
melded with the wealth of knowledge from people in the local community
and with Rwanda regionally. Over the course of these projects we’ve been
able to find really skilled workers. But what’s even more exciting is
that we’ve seen these people take those skills and find other jobs
because of the recognition they’ve received for the work on these
projects. We’ve seen that in different trades such as masonry, welding,
weaving, and pottery.
Alan Ricks: It reminds us that so much of the
architecture is about maximizing the potential of labor. And in order
for us to achieve high-quality results with limited resources, by
necessity our practice began with trying to see what high-skilled local
labor we could leverage to maximize the impact, the dignity, the beauty,
and the outreach this process could potentially have into the
community.
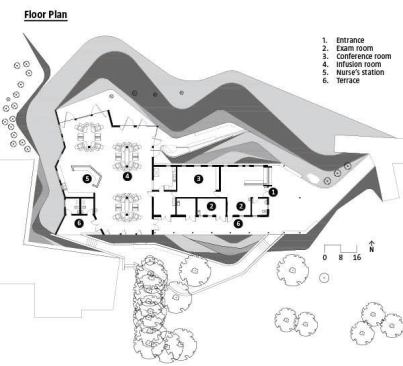
How did you focus on patient care in the design of the cancer center?
Sarah Mohland:
The infusion center is a place where patients spend six to eight hours
at a time receiving treatment, so we tried to make the space as
comfortable and peaceful as possible. The interior is a very bright
yellow and it creates a calm space. Patient care is centralized along
three infusion pods, and it allows for the patients to have visitors. A
chair provides seating for up to two family members. We emphasized
patient care by allowing for easy access for the physicians and the
nurses to reach them in a centralized place.
Murphy: There was potential here to take advantage
of this amazing landscape. By customizing the doors and opening the
façade, we knew we could create an open space for these patients to feel
dignity and respite. In order to open the view, we created a butterfly
roof, which is also represented in the Y-shape of the columns
themselves. So there’s a thematic strategy in the engineering as well as
the holding up the roof of this kind of lifting, this branching up, in
order to create a more lively open space.
There’s a lot we can learn about medical space in the U.S. from what is
being prototyped in Rwanda. Open air, leveraging the environment—those
are things that have been largely designed out of U.S. medical
facilities. I think it behooves us to remember how those kinds of open
air environments can also be very valuable and protective and safe for
patients.
Describe the structure and the building materials. Were there
any unique decisions that you had to make because of climate or culture?
Murphy:
The way we approach every project is through an initial immersion. The
idea is not only to uncover the challenges on the project, but also to
uncover opportunities that we can leverage to amplify the impact. When
Rwanda labor costs for a good-paying job are still low relative to
materials, it creates a real opportunity for customization on a larger
scale. And so we said, “Okay, we’re creating this custom hand-sawed wood
formwork, and isn’t this a chance to do something more unique with the
structure of the space to give it a character that reflects that
opportunity?” And so we worked with our Rwanda engineering team to look
at how we could optimize the structure to create this spacious, airy
open space while using the form of the structure to highlight that.
It’s clear that your work in Butaro shows the value that good
design can bring to the country in a way that is often not appreciated
in the developed world.
Murphy: I think we
forget that it’s possible to design an architecture that improves
people’s lives first and foremost, rather than the aspirational object
that could be value engineered out. Our system is so overdesigned in
terms of liabilities and litigiousness that it’s hard to sift through it
to see the value and the potential that’s right in front of us to
change the built environment we’re already living in. I think working in
Rwanda shows us that it’s not only possible, it’s absolutely
imperative. If we don’t do it, we’re going to see our infrastructure
continue to corrode and fall apart in the U.S. We’re going to see job
opportunities that are lost. We’re going to see a lack of investment in
health and safety in our communities if we don’t think about the
infrastructure we live within as part of the methodology to improve our
lives.
In other words, the U.S. can learn a lot from Rwanda if we take these things seriously.
Murphy: I really believe that. —Thomas Fisher