
It has become clear over the past few weeks that the United States was not—and is not—prepared to deal with a global pandemic. Neither our health care systems nor our medical facility infrastructure were designed to handle the influx of critically ill patients anticipated by cities as COVID-19 spreads through the population.
First responders are working tirelessly to provide medical care, source critical medical equipment, and encourage the general public to stay home and help flatten the curve. But cities are scrambling to find space to treat overflow COVID-19 patients and house health care personnel. In New York City, the 1.8 million-square-foot Javits Convention Center was converted into a 1,000-bed facility; erection of a temporary field hospital in Central Park is underway, with more spaces planned. Naval hospital ships are already docked and accepting patients in New York and Los Angeles, where city officials are also working to convert the LA Convention Center into a 2,600-bed facility. Hotels and university dorms across the nation are being offered for increased capacity. After launching pilot programs in Italy and France, Airbnb has announced it will aim to provide housing to 100,000 first responders in the U.S.
While these and many other cities are turning to the Army Corps of Engineers, the Federal Emergency Management Agency, and local response teams to plan and execute the reuse of alternative facilities, architects, designers, and engineers are also volunteering or being brought into the fold for their expertise. ARCHITECT spoke with teams from SmithGroup, Perkins and Will, CannonDesign, and NBBJ about how they are assisting with these efforts in this unprecedented time.
Understanding the Challenges
According to NBBJ principal Bryan Langlands, AIA, the greatest issues facing first responders and healthcare facility managers are “capacity, equipment, and staff,” he says. “All three are required to deliver appropriate care to patients in a manner that is efficient and safe for staff.”
However, unlike China, South Korea, and other countries that have instituted nationwide protocols for addressing the crisis, the U.S. has largely left facility planning, equipment sourcing, and overall pandemic response to individual states. With varying health care systems and building codes at play in each state, professionals are acknowledging that a universal solution to increase COVID-19 infrastructure is virtually impossible. “Part of the challenge in this country right now is that we have 50 ways of doing health care and 50 different ways of regulating health care,” explains Juliet Rogers, president of CannonDesign’s Blue Cottage health care planning practice. “Whereas we can put out information and ideas, we can’t necessarily call them recommendations, because they might not meet the codes in every state.”
To best understand the challenges different health care systems are facing, Rogers started by picking up the phone and calling existing or former clients to offer support. “These teams have had their incident command centers set up since early March and they’re exhausted,” Rogers says. “So, we’re just trying to provide extra sets of hands, eyes, ears, and ideas wherever we can.”
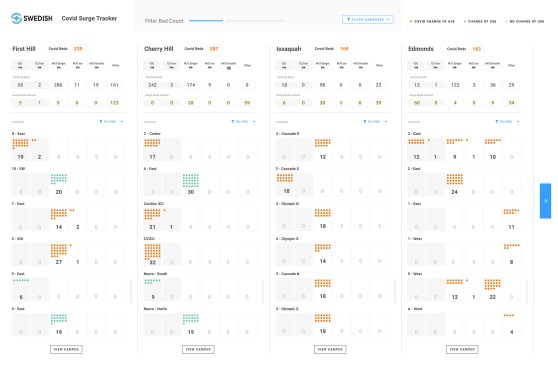
For Seattle-based Perkins and Will principal Brad Hinthorne, AIA, assisting his clients in the Pacific Northwest—one of the first regions in the U.S. to experience a surge of COVID-19 patients—had little to do with design plans or construction in the early phases. Instead, hospital systems needed help organizing incoming data. “It really started with helping them get real-time data of how many places they could accommodate cases across their system,” Hinthorne says. To address this need, Perkins and Will created dashboards with “graphics that their C-suite could use in their command center to help manage the day-to-day work they were doing,” he says.
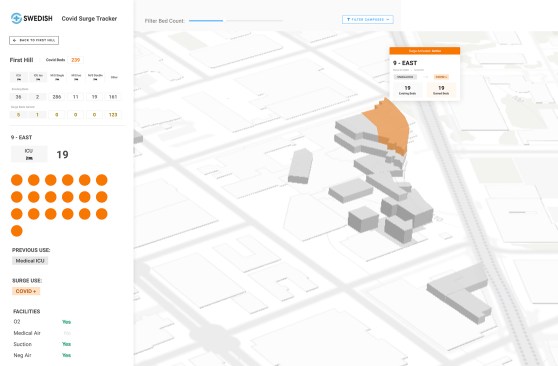
Perkins and Will
Perkins and Will
Perkins and Will has also been fielding calls from health care clients “asking about how they can rework their MEP systems to make more patient rooms negative pressure,” says Marvina Williams, a registered nurse and health care operations specialist based in Perkins and Will’s Atlanta office. “They’re looking closely at how they can turn patient floors into negative pressure floors for really sick patients that have COVID-19 symptoms.”
Finding Solutions
Some hospitals were designed with the capacity to convert emergency rooms and non-critical care units to rapid-response and intensive care units. As an example, Williams points to the Rush University Medical Center in Chicago, which Perkins and Will designed with bioterrorism and surge preparedness. At Rush, doors to the ambulance bay can be closed to create a COVID-19 triage area to limit exposure to other emergency room patients. In case of a surge, the ER was designed to be acuity adaptable with structural columns fitted with electrical outlets and to handle medical gases. “The emergency room is divided into three zones and set up for cordoned-off negative-pressure areas,” Williams explains. “If 20 beds are needed for negative pressure they can do that. If they need 20 more, they can continue on.”
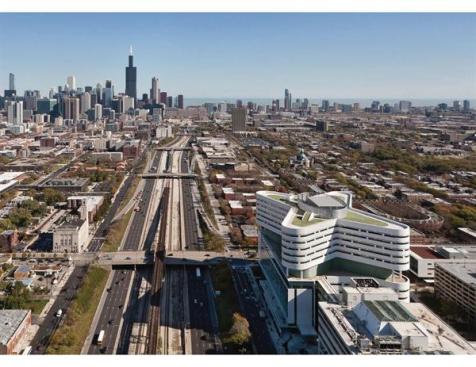
Rush University Medical Center
However, the reality of transforming or creating more urgent-care facilities quickly to address COVID-19 surges is sobering. “Even if you wanted to do it by hospital room, the majority of the infrastructure on a campus is not designed for these types of loads,” Hinthorne explains. Instead, cities and hospital systems are setting out to optimize existing infrastructure and invest in alternative spaces for less critically ill patients. “Creating critical care settings outside of a hospital is incredibly challenging,” Rogers says. “We would get more value from using non-hospital settings for supporting lower acuity care, for supporting non-infectious care, for supporting staff who need a place to sleep.”
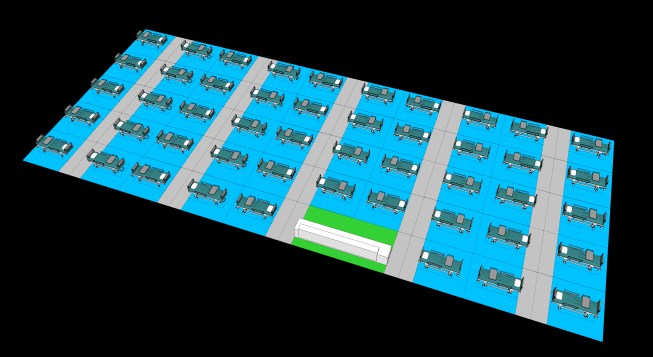
This is exactly the approach that Los Angeles has adopted in its conversion of its convention center into a 2,600-bed “hospital decompression site” for COVID-19 patients, with the help of SmithGroup. The partnership began with an urgent text from Christopher Hawthorne—chief design officer of the city and former Los Angeles Times architecture critic—to SmithGroup vice president Bonnie Khang-Keating seeking speculative test-fit plans for the space. “We pulled a team of about a dozen architects and engineers together to jump into this exercise of using the LA Convention Center to free up beds in the hospitals for those high acuity patients, transferring patients with low acuity to the convention center,” Khang-Keating explains. In 24 hours, the team led by Francisco Owens, AIA, put together plans for a maximum capacity, low-acuity care facility.
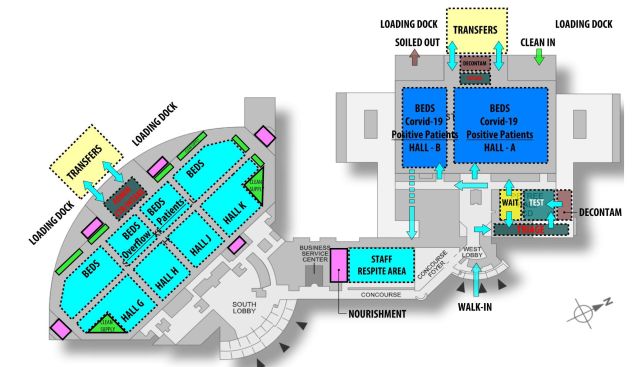
SmithGroup

SmithGroup
Potential LA Convention Center South Hall layout
“We engaged with SmithGroup to understand what is a smart layout for this type of facility to be able to maximize the space,” says Jasson Crockett, manager of economic policy in the mayor’s office of economic development. “It was really helpful to be able to turn to SmithGroup and have them bring in the expertise from the architectural side, the electrical considerations, and HVAC considerations, especially given the concerns around COVID-19’s ability to spread through HVAC within a building. These are things that we probably may have gotten to, but it would have taken us a lot longer to figure out.”
SmithGroup
Lessons to Learn
While it is difficult to conceive of a reality after this pandemic passes, these teams are also tracking their findings and best practices to share with cities experiencing later COVID-19 surges and for future design projects. Perkins and Will’s client Providence Health & Services, which operates 50 hospitals in Alaska, Washington, Oregon, California, Montana, New Mexico, and Texas, is already sharing relevant data and lessons across their various facilities.
Additional design interventions and strategies are sure to follow as information on disease transmission becomes more readily available. “Our next focus is to reduce the amount of items to touch in the first place,” Langlands says. “This means, where possible, removing unnecessary equipment and adapting to more hands-free technologies to do things like turn on open and close doors, turn lights on and off, and open garbage cans. Smooth surfaces without crevices are important, along with exploring materials with inherent properties that have shown promise in providing environments that are hostile to viruses and organisms, like copper and silver.”
“As we’re planning the next wave of projects, we can all pretty much guarantee that there’s going to be a lot of discussion on what we should be doing differently to adapt or when we create new facilities,” Hinthorne says.
To receive our latest coverage of COVID-19 in your inbox, subscribe to ARCHITECT newsletters.


